
ALERT!
This site is not optimized for Internet Explorer 8 (or older).
Please upgrade to a newer version of Internet Explorer or use an alternate browser such as Chrome or Firefox.
Beyond Zone 0 AMDS Implantation
Cavozza C, Gherli R, Pellegrino P, et al. Beyond Zone 0 AMDS Implantation. February 2026. doi:10.25373/ctsnet.31298020
When the initial tear is located within the aortic arch, the surgical strategy often involves a more comprehensive repair (1, 2). Surgical procedures involving the transverse aortic arch are particularly complex (3, 4, 5, 6, 7, 8). This evolving landscape has led to various innovative strategies to improve patient outcomes (7, 8, 9). The Ascyrus Medical Dissection Stent (AMDS) has been developed to address issues related to the downstream thoracic aorta (10, 11). Positioned proximal to the brachiocephalic trunk (zone 0), this stent works in concert with standard ascending aorta replacement to enhance surgical outcomes, improving positive aortic remodeling and reducing malperfusion (5) (Figure 1).
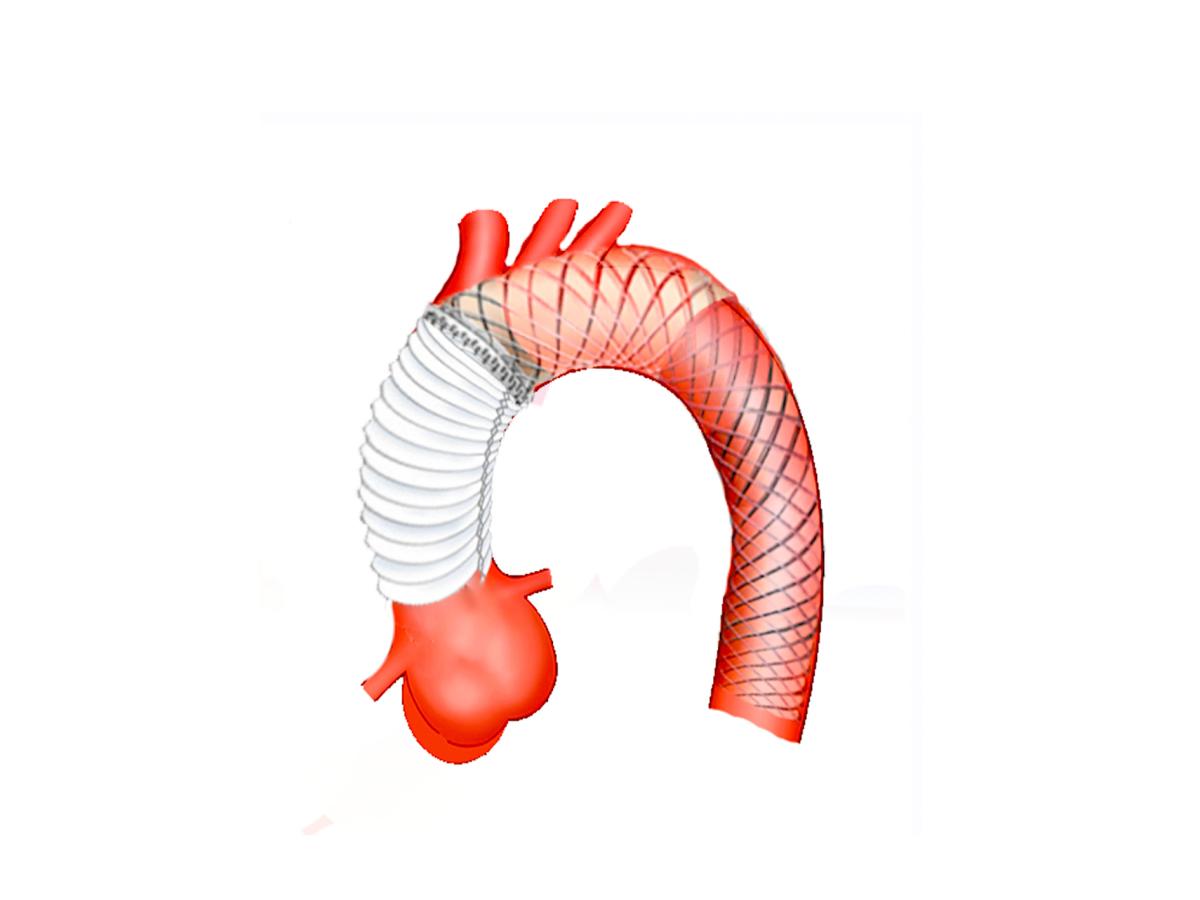
Figure 1: This figure illustrates the AMDS implant in zone 0.
By extending the surgical implantation beyond zone 0, surgeons can enhance the likelihood of successful outcomes (5) (Figure 2).
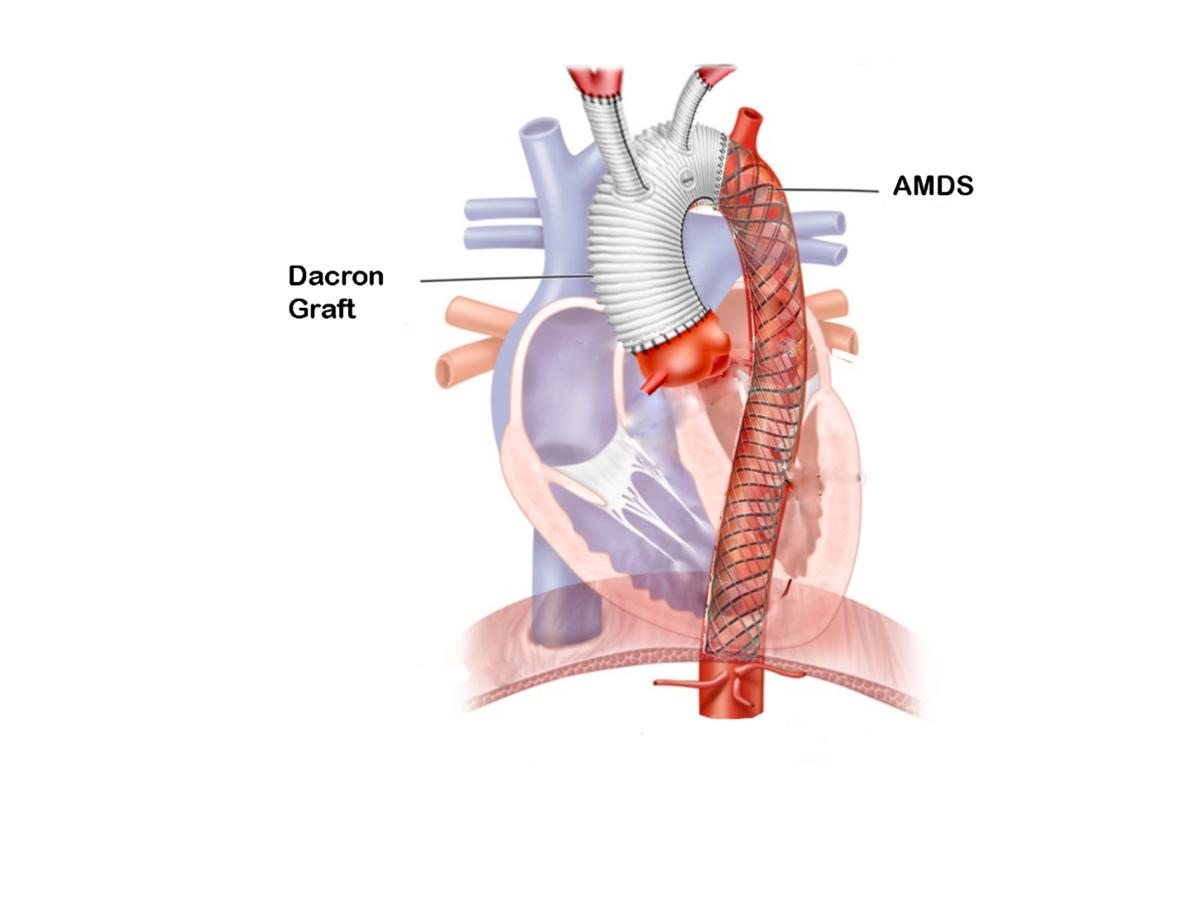
Figure 2: This figured illustrates the AMDS implant in zone 2.
The author’s preliminary experience suggests that this technique may offer significant benefits, such as:
- Simpler distal anastomosis
- Ability to approach the most complex arch tears
- Shorter aortic cross-clamp (ACP) times compared to total arch frozen elephant trunk (FET)
- Potential for TEVAR options in the future
- Reduced risk of recurrent laryngeal nerve injury
- No surgical involvement of the left subclavian artery.
A 68-year-old male presented with chest pain and numbness in the left lower extremity.
The computed tomography (CT) angiogram demonstrated an acute aortic dissection, classified as non-A non-B (TA, E2, M3). The patient was transferred to the operating room.
After performing a midline skin incision and before pericardiectomy, the innominate artery was exposed and encircled with an umbilical tape. In the same fashion, the left carotid artery was prepared.
Two simple box-shaped stitches of 5-0 polypropylene were placed side by side but in opposite directions, buttressed with the same Teflon-felt pledgets, on the anterior wall of the innominate artery (Figure 2) to allow direct insertion of the cannula after heparin administration.
The purse strings were snugged, and the cannula was affixed to the tourniquets (Figure 3). After venous cannulation, cardiopulmonary bypass was started, and the patient was cooled to 28° C. Cerebral perfusion was monitored by near-infrared spectroscopy (NIRS).
The ascending aorta was cross-clamped just proximal to the innominate artery. Myocardial preservation was achieved through the antegrade infusion of cold histidine-tryptophan-ketoglutarate (HTK) solution.
A transverse aortotomy was performed, and the entry tear was not identified in the aortic root or ascending aorta.
The left common carotid artery was divided from the aorta using a surgical stapler. The artery was connected to a Dacron graft and cannulated using a Y-line from the arterial line.
The cardiopulmonary bypass (CPB) flow was stopped, and the innominate artery was separated from the aorta with the same surgical stapler. The clamp was removed, and the aortic arch was opened. Selective bilateral antegrade brain perfusion was started at a rate of 10 mL/kg/min.
A tear near the left subclavian artery was closed with two simple stitches of 4-0 polypropylene, buttressed with the Teflon-felt pledgets, placed from inside to outside the aorta.
A Teflon felt strip was positioned circumferentially on the outer portion of the distal aorta and sewn in place with three single 3-0 Prolene stitches.
The AMDS was then implanted and sewn in place with mattress 3-0 Prolene sutures, incorporating the stent graft on the inside of the aorta.
A balloon occlusion catheter was inserted into the descending thoracic aorta through the AMDS, which allowed antegrade perfusion of the lower half of the body at a rate of 500 ml/min, with the system connected to a cardioplegia pump while NIRS was used to monitor the brain and lower back (Figure 3).

Figure 3: This figure shows NIRS monitoring the brain and lower back.
A quadrifurcated graft with three arch branches and a side perfusion limb was modified by excising the distal end and subclavian branch. It was then sewn end-to-end to the distal transverse arch, incorporating the stent graft, native aortic wall, and felt strip using 3-0 Prolene sutures. Once the distal anastomosis was completed, the arterial cannula was placed into the side limb of the arch graft, and CPB was restarted. The proximal anastomosis with the ascending aorta was performed end-to-end using 3-0 Prolene sutures. End-to-end anastomosis of the arch branches to the left common carotid and innominate arteries was performed with 5-0 Prolene sutures. The postoperative course was uneventful and the patient was discharged on postoperative day 10. The predischarge CT carotid angiography showed no residual antegrade flow in the false lumen across the arch, with well-restored flow in the right subclavian and carotid arteries, and normal perfusion of the left subclavian artery.
References
- Mitchell, R. Scott. "Acute aortic dissections with entry tear in the aortic arch: International Registry of Acute Aortic Dissection to the rescue." The Journal of Thoracic and Cardiovascular Surgery 156.5 (2018): 1794.
- Sievers HH, Rylski B, Czerny M, Baier ALM, Kreibich M, Siepe M, et al. Aortic dissection reconsidered: type, entry site, malperfusion classification adding clarity and enabling outcome prediction. Interact Cardiovasc Thorac Surg. (2020) 30:451–7. doi: 10.1093/icvts/ivz281
- Rylski B, Beyersdorf F, Kari FA, Schlosser J, Blanke P, Siepe M. Acute type A aortic dissection extending beyond ascending aorta: Limited or extensive distal repair. J Thorac Cardiovasc Surg. (2014) 148:949–54; discussion 54. doi: 10.1016/j.jtcvs.2014.05.051
- Czerny M, Rylski B. Acute type A aortic dissection reconsidered: it’s all about the location of the primary entry tear and the presence or absence of malperfusion. Eur Heart J. (2021) 43:53–55. doi: 10.1093/eurheartj/ehab664
- Mehdiani, Arash, et al. "Early results of a novel hybrid prosthesis for treatment of acute aortic dissection type A with distal anastomosis line beyond aortic arch zone zero." Frontiers in Cardiovascular Medicine 9 (2022): 892516.
- William C. Frankel, Susan Y. Green, Vicente Orozco-Sevilla, Ourania Preventza and Joseph S. Coselli. Contemporary Surgical Strategies for Acute Type A Aortic Dissection. Semin Thoracic Surg 32:617629
- Shrestha M, Haverich A, Martens A. Total aortic arch replacement with the frozen elephant trunk procedure in acute DeBakey type I aortic dissections. Eur J Cardiothorac Surg. (2017) 51:i29–34. doi: 10.1093/ejcts/ezw341
- Rylski B, Milewski RK, Bavaria JE, Vallabhajosyula P, Moser W, Szeto WY, et al. Long-term results of aggressive hemiarch replacement in 534 patients with type A aortic dissection. J Thorac Cardiovasc Surg. (2014) 148:2981–5. doi: 10.1016/j.jtcvs.2014.05.093
- Xue, Yunxing, et al. "Different aortic arch surgery methods for type A aortic dissection: clinical outcomes and follow-up results." Interactive cardiovascular and thoracic surgery 31.2 (2020): 254-262.
- Bozso SJ, Nagendran J, MacArthur RGG, Chu MWA, Kiaii B, El-Hamamsy I, et al. Dissected aorta repair through stent implantation trial: Canadian results. J Thorac Cardiovasc Surg. (2019) 157:1763–71
- Szeto, Wilson Y., et al. "A novel hybrid prosthesis for open repair of acute De Bakey type I dissection with malperfusion: Early results from the PERSEVERE trial." The Journal of Thoracic and Cardiovascular Surgery 170.1 (2025): 114-123.
Disclaimer
The information and views presented on CTSNet.org represent the views of the authors and contributors of the material and not of CTSNet. Please review our full disclaimer page here.



